Written by: Vihan DeSilva with Dr. Nabil Ebraheim
Spinal stenosis is a diagnosis mainly made through history and CT/MRI imaging as physical exam findings can be normal namely in lumbar spinal stenoses. A common finding along with painful extension of the spine and decreased lumbar lordosis is narrowing of the spinal foramina, but diagnosis is made when patients present with neurogenic claudication and/or cervical myelopathy. The cause may be congenital or acquired through, for example, endocrinopathies, calcium metabolism disorders, inflammatory diseases, and infectious diseases.1,2 There are other diseases that produce similar symptoms that should be considered in the differential diagnosis of spinal stenosis including metastatic disease, hip disease, peripheral neuropathy, disc herniation, and vascular disease/ vascular claudication.2 The rest of this article will be a discussion on how to differentiate spinal stenosis from these other conditions.
Patients’ pain may be metastatic if it is constant and worse at night or is unresolved even after previous attempts at treatment. Metastatic origin of pain should also be considered in patients who have a cancer/ cancer treatment history or experience fatigue, malaise, unintentional weight loss, or nonspecific symptoms.2,3
Distinguishing
hip disease (ie. osteoarthritis) pain from lumbar stenosis pain can be
challenging because the two ailments can coexist in a condition known as
hip-spine syndrome. The location of the pain can be helpful in identifying the
primary pain generator: hip pain can be felt in the groin, lateral hip,
posterior hip, or near the spine and SI joint. Internal rotation of
the hip can also be compromised in hip disease.2,4 Another way to
isolate the pain generator is to inject the hip with steroid and observe.
Worsening symptoms could indicate pain coming from lumbar stenosis. However,
increased activity of the patient may also cause pain in related structures
after the initial injection if it was successful in treating pain from underlying
hip osteoarthritis.2

Peripheral
neuropathy can also coexist with lumbar stenosis and may further complicate the
differential diagnosis of spinal stenosis. EMG studies could aid in discerning stenosis
from peripheral neuropathy and motor neuron disease.5 Certain
clinical findings may also be useful. Bilateral burning foot pain at night is a
distinguishing feature of peripheral neuropathy whereas unilateral leg pain
with activity that is relieved by sitting is characteristic of lumbar stenosis/
radiculopathy. Additionally, sensory testing that demonstrates a dermatomal
pattern indicates a problem in the spinal root whereas a glove and stock
pattern would hint towards peripheral neuropathy.1,2
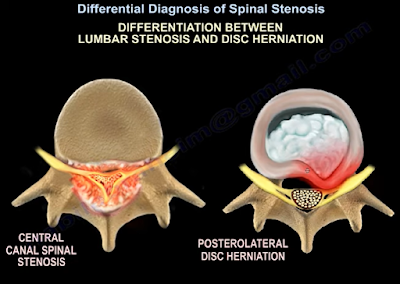
Disc
herniation should also be considered against spinal stenosis as a possible
source of pain. Location of pain can once again help in identifying the correct
source. According to one comparative study, herniations tend to produce leg pain
in the anterior thigh, anterior knee, and shin whereas posterior knee pain was common
with stenosis.6 Furthermore, characteristics of stenosis include
bilateral, nonspecific leg pain that is generally above the knee and rarely
produces a positive straight-leg test. In contrast, herniation causes
unilateral pain along the dermatome of the affected nerve root along with a
positive straight-leg test.2
Vascular
disease should be ruled out as well when considering a spinal stenosis
diagnosis. One main distinguishing principle is that vascular disease produces vascular
claudication whereas spinal stenosis produces neurogenic claudication. These
two different types of claudication have different clinical sequelae. For
instance, the distance a patient can walk before feeling symptoms is more
variable with neurogenic claudication than with vascular claudication and
uphill walking is better tolerated only with neurogenic claudication. Sitting
attenuates neurogenic claudication symptoms whereas both sitting and standing
still may ease vascular claudication symptoms.7 Vascular pain
travels from distal sites to proximal ones whereas neurogenic pain goes from
proximal to distal. Unlike vascular claudication, bilateral pedal pulses are
normal with neurogenic claudication. Unlike spinal stenosis, vascular disease
may produce lower extremity ulcers, hair loss, edema, and skin changes.2 Lastly,
postural adjustments, such as flexion of the spine, ease stenosis claudication
symptoms due to relief of pressure on the nerve roots. This is not true in
vascular disease. This is also why a bicycle test relieves stenosis pain while
making vascular pain worse.8
Other rarer considerations
include spinal arteriovenous malformations, tumors of the cauda equina, and differential
diagnosis of myelopathy (ALS, multiple sclerosis, or subacute combined
degeneration).1 Once a spinal stenosis diagnosis is made, the
condition can be managed non-surgically with drugs, physiotherapy, and
injections or surgically through decompression, spinal fusion, or interspinous
spacer devices.9 Evidence is still being gathered on effectiveness
and outcomes for all these non-surgical and surgical treatment options though.
References
1. Melancia JL, Francisco AF, Antunes JL. Spinal stenosis. Handb Clin Neurol. 2014;119:541-9.
2. Ebraheim N. Differential Diagnosis of Spinal Stenosis [Internet]. Toledo (OH): University of Toledo Medical Center, Department of Orthopedic Surgery; 2021 Jun 25. Available from: https://www.youtube.com/watch?v=eYxPmrnfjfA&ab_channel=nabilebraheim.
3. Dodwad SM, Savage J, Scharschmidt TJ, Patel A. Evaluation and treatment of spinal metastatic disease. Cancer Treat Res. 2014 Jul 29;162:131-50.
4. Brown MD, Gomez-Marin O, Brookfield KF, Li PS. Differential diagnosis of hip disease versus spine disease. Clin Orthop Relat Res. 2004 Feb;419:280-4.
5. Plastaras CT. Electrodiagnostic challenges in the evaluation of lumbar spinal stenosis. Phys Med Rehabil Clin N Am. 2003 Feb;14(1):57-69.
6. Rainville J, Lopez E. Comparison of radicular symptoms caused by lumbar disc herniation and lumbar spinal stenosis in the elderly. Spine (Phila Pa 1976). 2013 Jul 1;38(15):1282-7.
7. Genevay S, Atlas SJ. Lumbar spinal stenosis. Best Pract Res Clin Rheumatol. 2010 Apr;24(2):253-65.
8. Binder DK, Schmidt MH, Weinstein PR. Lumbar spinal stenosis. Semin Neurol. 2002 Jun;22(2):157-66.
9. Lurie J, Tomkins-Lane C. Management of lumbar spinal stenosis. BMJ. 2016 Jan 4;352:h6234.