Written by Ryan Jones with Dr. Nabil Ebraheim
Neck and upper extremities spine examination or cervical spine physical examination involves assessment of vertebrae C3-T2, cranial nerve roots C4-T1, and all the muscles innervated by these nerve roots along with the muscles associated with basic neck movement. This examination follows the typical pattern of orthopedic examination of inspection, palpation, range of motion, neurological evaluation, and special tests1.
Inspection
Check for any visual deformities
or abnormal anatomical alignments in the coronal and sagittal plane including
typical cervical lordosis and thoracic kyphosis1. Also, look for any
surgical scars, skin defects like café au lait spots, or muscular atrophy2.
Muscular atrophy can present as shoulder imbalance, scapular winging, or a
general unilateral reduction in size of muscles of the upper extremities.
Palpation
Palpate for local tenderness
along the spinal axis while also looking for any asymmetry2. This
includes palpations of the spinous processes and facet joints of the vertebrae
along with palpation of the scapula to look for any asymmetry. Palpate the
paraspinal muscles while looking for any tenderness or asymmetry. The muscles
of importance include the trapezius, rhomboids, and levator scapulae muscles1,3.
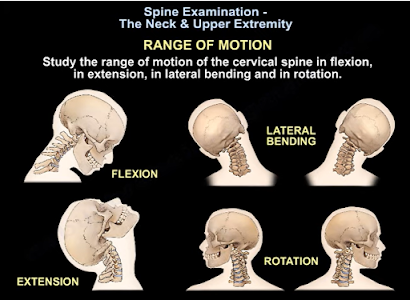
Range of Motion
Range of motion
for the cervical spine involves checking cervical flexion (normal = 50),
extension (normal = 60), rotation (normal = 80), and lateral bending (normal =
45)2. A thorough range of motion examination should also be done for
the shoulder due to the extensive nerve root innervation. Shoulder range of
motion involves testing abduction (normal = 180), adduction (normal = 45),
flexion (normal = 90), extension (normal = 45), internal rotation (normal =
55), and external rotation (normal = 45)4. Any abnormalities in
range of motion can be indicative of muscular or neurological pathologies.
Neurological Examination
Test the motor ability and
strength of the muscles associated with each cranial root for strength by
grading it 0-V based on the muscle manual testing grading system2,3.
Any weakness is a sign of muscular or neurological pathology. Next, test for sensory
function for pain (with a paper clip) and light touch (finger) sensation at the
dermatome for each cranial nerve1. Any abnormalities may be a result
of neurological pathologies. Test the biceps reflex for C5, brachioradialis
reflex for C6, and triceps reflex for C7 cranial nerve root abnormalities1.
Special Tests
Use the following provocative
test to differentiate neck pathologies from other upper extremity:
·
Spurling’s test is indictive of acute
radioculopathy2.
·
Hoffman’s test is indictive of cervical
myelopathy2.
·
Lhermitte’s test is indicative of compression
and myelopathy of the cervical spine2.
·
Stretch test is indicative of brachial plexus
pathology.
·
Compression test is indicative of narrowing of
the neural foramen, facet joint pressure, or muscle spasms from the paraspinal
muscles3.
·
Observation of steppage, lateral, or wide-base
gait are all indicative of myelopathy or neurological pathology2.
Remember that an MRI may be
required to confidently differentiate between shoulder and neck pathologies1.
References
1.
Ebraheim N. Spine Exam & Upper Extremity –
Everything You Need to Know – Dr. Nabil Ebraheim [Internet]. Toledo (OH):
University of Toledo Medical Center, Department of Orthopedics; 2021 Aug 4
[cited 2021 Oct 23]. Available from: https://www.youtube.com/watch?v=hIiV-xi2TiE.
2.
Moore DW. Neck & Upper Extremity Spine Exam
[Internet]. Santa Barbara (CA): Santa Barbara Orthopedic Associates; 2021 June
27 [cited 2021 Oct 23]. Available from: https://www.orthobullets.com/spine/2001/neck-and-upper-extremity-spine-exam
3.
Iyer KM. Examination of the Cervical Spine. In:
Clinical Examination in Orthopedics. London: Springer; 2012. pp 97-107.
4.
Iyer KM. Examination of the Shoulder. In:
Clinical Examination in Orthopedics. London: Springer; 2012. pp 9-18.