The frozen shoulder can be
associated with diabetes or thyroid disease.
It may be the initial presenting symptom for these conditions. The exact details of this relationship remain
poorly understood. Ever patient with a
frozen shoulder should have the HbA1c and TSH levels tested. Also, check for arthritis, rheumatoid factors
and antinuclear antibodies. Most
patients with frozen shoulder are female between the ages of 40 and 60 years
old. And frozen shoulder, the patient
will lose both the active and the passive range of motion of the shoulder. The patient develops pain, which means that
there is inflammation with early fibrosis of the joint capsule, leading to
joint stiffness. The active and passive
global motion, especially external rotation, will be reduced compared to the
other side. The shoulder pain and motion
loss is usually not related to trauma.
It is an idiopathic process that results in shoulder pain and loss of motion
due to contracture of the capsule. The
essential lesion involves the coracohumeral ligament and the rotator
interval. The synovial inflammation and
capsular fibrosis results in pain and joint volume loss. Check for previous trauma or fractures. Rule out shoulder joint arthritis and rule
out posterior dislocation of the shoulder.
It can also occur post-surgery from a rotator cuff tear. It may also be associated with dupuytren
disease and cervical disc disease. Check
for medical comorbidities such as stroke or cardiac diseases. The x-ray will exclude trauma, malignancy, arthritis,
calcific tendinitis, impingement, and AC joint arthritis. And frozen shoulder, the humeral head will
remain in its normal location.
MRI
There is a space reduction in
the axillary recess. Rotator cuff
strength is normal by exam and on the MRI.
The pain and stiffness lasts beyond 6 months, then you can do
manipulation of the shoulder under anesthesia.
There is a 50% failure rate in diabetics. The diabetes is associated with a much worse
prognosis and poor outcome for surgical and nonsurgical treatment.
Treatment
·Nonoperative
oThis should be
done for at least 3 to 6 months.
oSupervised or
home-based capsular stretching program +/-intra-articular steroid joint
injection.
oNonsteroidal
anti-inflammatory medication
·Surgery
oCapsular release
(arthroscopic or open) and release the intra-articular and subacromial
adhesions.
oThe axillary
nerve may be injured during release of the capsule.
oUtilize surgery
in patients that have failure of initial conservative treatment for 3 months,
and the patient remains functionally limited.
Neck and upper extremities
spine examination or cervical spine physical examination involves assessment of
vertebrae C3-T2, cranial nerve roots C4-T1, and all the muscles innervated by
these nerve roots along with the muscles associated with basic neck movement.
This examination follows the typical pattern of orthopedic examination of inspection,
palpation, range of motion, neurological evaluation, and special tests1.
Inspection
Check for any visual deformities
or abnormal anatomical alignments in the coronal and sagittal plane including
typical cervical lordosis and thoracic kyphosis1. Also, look for any
surgical scars, skin defects like café au lait spots, or muscular atrophy2.
Muscular atrophy can present as shoulder imbalance, scapular winging, or a
general unilateral reduction in size of muscles of the upper extremities.
Palpation
Palpate for local tenderness
along the spinal axis while also looking for any asymmetry2. This
includes palpations of the spinous processes and facet joints of the vertebrae
along with palpation of the scapula to look for any asymmetry. Palpate the
paraspinal muscles while looking for any tenderness or asymmetry. The muscles
of importance include the trapezius, rhomboids, and levator scapulae muscles1,3.
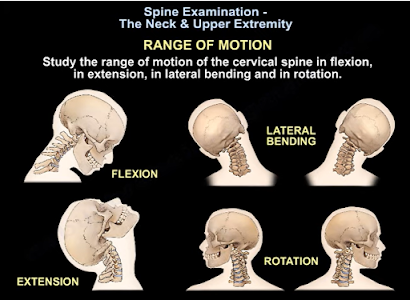
Range of Motion
Range of motion
for the cervical spine involves checking cervical flexion (normal = 50),
extension (normal = 60), rotation (normal = 80), and lateral bending (normal =
45)2. A thorough range of motion examination should also be done for
the shoulder due to the extensive nerve root innervation. Shoulder range of
motion involves testing abduction (normal = 180), adduction (normal = 45),
flexion (normal = 90), extension (normal = 45), internal rotation (normal =
55), and external rotation (normal = 45)4. Any abnormalities in
range of motion can be indicative of muscular or neurological pathologies.
Neurological Examination
Test the motor ability and
strength of the muscles associated with each cranial root for strength by
grading it 0-V based on the muscle manual testing grading system2,3.
Any weakness is a sign of muscular or neurological pathology. Next, test for sensory
function for pain (with a paper clip) and light touch (finger) sensation at the
dermatome for each cranial nerve1. Any abnormalities may be a result
of neurological pathologies. Test the biceps reflex for C5, brachioradialis
reflex for C6, and triceps reflex for C7 cranial nerve root abnormalities1.
Special Tests
Use the following provocative
test to differentiate neck pathologies from other upper extremity:
·Spurling’s test is indictive of acute
radioculopathy2.
·Hoffman’s test is indictive of cervical
myelopathy2.
·Lhermitte’s test is indicative of compression
and myelopathy of the cervical spine2.
·Stretch test is indicative of brachial plexus
pathology.
·Compression test is indicative of narrowing of
the neural foramen, facet joint pressure, or muscle spasms from the paraspinal
muscles3.
·Observation of steppage, lateral, or wide-base
gait are all indicative of myelopathy or neurological pathology2.
Remember that an MRI may be
required to confidently differentiate between shoulder and neck pathologies1.
References
1.Ebraheim N. Spine Exam & Upper Extremity –
Everything You Need to Know – Dr. Nabil Ebraheim [Internet]. Toledo (OH):
University of Toledo Medical Center, Department of Orthopedics; 2021 Aug 4
[cited 2021 Oct 23]. Available from: https://www.youtube.com/watch?v=hIiV-xi2TiE.
2.Moore DW. Neck & Upper Extremity Spine Exam
[Internet]. Santa Barbara (CA): Santa Barbara Orthopedic Associates; 2021 June
27 [cited 2021 Oct 23]. Available from: https://www.orthobullets.com/spine/2001/neck-and-upper-extremity-spine-exam
3.Iyer KM. Examination of the Cervical Spine. In:
Clinical Examination in Orthopedics. London: Springer; 2012. pp 97-107.
4.Iyer KM. Examination of the Shoulder. In:
Clinical Examination in Orthopedics. London: Springer; 2012. pp 9-18.
Bursas are synovium-lined, sac-like
structures located throughout the body between skin and tendon or tendon and
bone (1,2). The main function of bursa is to reduce the friction between areas
of movement and some common locations are the shoulder, knee, hip, and elbow
(1). When these areas become swollen or inflamed it is known as bursitis.
During this abnormality the bursa will enlarge with fluid causing any movement
against or direct pressure upon the area to produce pain for the patient (2).
There are many causes of bursitis that
one should be aware of, five of which are prolonged pressure, trauma, sepsis,
autoimmune conditions, and idiopathic origins. Prolonged pressure is when the
bursa is stressed between a hard surface and bony prominence. Examples of this
prolonged pressure include over-use of the area with repetitive motions,
frequently resting one’s elbow on their desk, and working on one’s knees
without adequate padding. Traumatic bursitis is caused when direct pressure is applied
to the bursa, often unknowingly as it may have seemed benign at the time (2). Traumatic
bursitis does put the patient at risk of developing septic bursitis, often
difficult to distinguish against aseptic bursitis, which is most induced by
invasive procedures (2,3). Staphylococcus aureus causes roughly 80% of
septic bursitis through what is believed to be a direct inoculation, instead of
a hematogenous route due to the poor blood flow seen to bursas (4). Bursitis
can also be caused by autoimmune conditions such as rheumatoid arthritis,
osteoarthritis, systemic lupus erythematosus, scleroderma, spondyloarthropathy,
and gout. The last common cause of bursitis is idiopathic in origin (2).
Bursitis can be broken up further to
acute bursitis and chronic bursitis. Acute bursitis is typically caused by trauma,
infection, or crystalline joint disease resulting in pain on palpation of the
bursa as well as a decrease in range of motion that is secondary to pain. Whereas
chronic bursitis is typically caused by inflammatory arthropathies, repetitive
motions, or microtraumas most often causing painless swelling and thickening of
the bursa. Examination of the skin is an important distinguishing factor for
acute and chronic bursitis as trauma, erythema, and warmth should all be
evaluated to make a proper diagnosis (2).
Diagnosis of many types of bursitis
can be made clinically without further studies, however in the case of trauma,
concern for foreign bodies, or fractures imaging can play an important role in
diagnosis. Basic plain film imaging can be used when evaluating a superficial
bursa however, for a deeper bursa MRI and ultrasound can be used (1).
Ultrasound will also provide the added benefit of showing real-time images to
observe changes in active and passive movements (2). When evaluating an
inflamed bursa, aspiration is a critical tool to distinguish between septic and
aseptic bursitis as the aspirated fluid should be sent for a basic cell count
and cell cultures (3).
Treatment for bursitis depends on the
type and causative agent as most bursitis will heal on their own without
intervention. To combat the patient’s pain, bursitis can be treated with a
conservative treatment plan involving rest, ice, compression, and elevation as
well as NSAIDS and/or acetaminophen for pain (2). With deeper bursitis
corticosteroid injections can provide symptomatic relief however, this course
of treatment is not recommended for superficial bursa and can delay the
diagnosis of another condition such as a tear. Physical therapy is another
important treatment method to strengthen the muscles that support the area
around the bursa (2). For septic bursitis the typical course of treatment is oral
antibiotics as an outpatient but systemic IV antibiotics may be needed if signs
of widespread sepsis are present (4). The last line of treatment is surgery
which is most often used only as a last resort when all other conservative
treatment methods fail (2).
References
1.Chatra PS. Bursae around the knee joints. Indian J Radiol Imaging. 2012 Jan;22(1):27-30. doi: 10.4103/0971-3026.95400. PMID: 22623812; PMCID: PMC3354353.
2.Williams CH, Jamal Z, Sternard BT. Bursitis. [Updated 2021 Aug 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK513340/
3.Aaron, Daniel L. MD; Patel, Amar MD; Kayiaros, Stephen MD; Calfee, Ryan MD Four Common Types of Bursitis: Diagnosis and Management, American Academy of Orthopaedic Surgeon: June 2011 - Volume 19 - Issue 6 - p 359-367
4.Cea-Pereiro JC, Garcia-Meijide J, Mera-Varela A, Gomez-Reino JJ. A comparison between septic bursitis caused by Staphylococcus aureus and those caused by other organisms. Clin Rheumatol. 2001;20(1):10-4. doi: 10.1007/s100670170096. PMID: 11254233.
While some people know what Ehlers-Danlos Syndrome (EDS) is, not many know that it is actually a group of 13 different disorders or types. One of the most prevalent types is Hypermobile Ehlers-Danlos Syndrome (hEDS), accounting for 80-90% of EDS cases [1]. The Ehlers-Danlos Syndromes are defined as inherited connective tissue disorders, affecting structural proteins (namely collagen) that leads to joint hypermobility, skin hyperextensibility, and tissue fragility [2]. hEDS is the only EDS subtype that does not have a currently known genetic basis, though it is a hereditary disorder with autosomal dominant inheritance pattern [2]. Therefore, hEDS is in part a diagnosis of exclusion, as genetic testing can be done for the other subtypes.
The Ehlers-Danlos Syndromes as whole are related to the Joint Hypermobility Spectrum, a spectrum of disorders intended to classify different severities of Hypermobility Spectrum Disorders (HSD). At the most extreme end of the hypermobile spectrum lies hEDS [3]. hEDS differs from the other EDS subtypes in its presentation as well. hEDS includes general joint hypermobility (GJH) but has less severe skin involvement compared to classical or vascular EDS types [1]. Easy bruising and impaired wound healing are also common. The definition of hEDS has evolved to include chronic pain and chronic fatigue as common presentations in those affected by the disease. The current diagnostic criteria include confirmation of GJH using the Beighton scoring system, positive musculoskeletal and pain symptoms or family history, and exclusion of other EDS subtypes or HSDs [4].
(Visit this link for the full diagnostic criteria of hEDS)
Apart from acute complications such as dislocation and subluxation, hEDs treatment revolves around chronic pain management and prevention of complications [1]. Acute exacerbations should be treated accordingly using joint reduction techniques and acute pain management. Physical therapy can be used to increase joint stability using low resistance exercises and stretching to increase muscle tone, thereby reducing the chance of acute joint injury. Patients should generally avoid hyperextension and high impact exercise. Oral acetaminophen, NSAIDs, and COX-2 inhibitors can be used as analgesics for chronic pain, as well as after acute injury. Cannabinoids can be considered for chronic pain, but opiates should rarely be used. If an hEDS patient must undergo surgery, careful technique should be used to minimize the wound site and promote healing. In summary, it is important to understand hEDS and how it differs from EDS and other HSDs to properly diagnose and treat patients.
References
1.Tinkle B, Castori M, Berglund B, Cohen H, Grahame R, Kazkaz H, et al. Hypermobile Ehlers-Danlos syndrome (a.k.a. Ehlers-Danlos syndrome Type III and Ehlers-Danlos syndrome hypermobility type): Clinical description and natural history. American Journal of Medical Genetics Part C: Seminars in Medical Genetics. 2017 Feb 1;175(1):48–69.
2.The Types of EDS [Internet]. The Ehlers Danlos Society. 2017. Available from: https://www.ehlers-danlos.com/eds-types/
3.What are the hypermobility spectrum disorders? [Internet]. The Ehlers Danlos Society. 2017. Available from: https://www.ehlers-danlos.com/what-is-hsd/
4.Forghani I. Updates in Clinical and Genetics Aspects of Hypermobile Ehlers Danlos Syndrome. Balkan Medical Journal. 2019 Jan 10;36(1):12–6.
Fractures of the Calcaneus: Everything You Need to Know
Written by Dominic Ruwe and Dr. Nabil Ebraheim
Fractures of the calcaneus can be open or closed.1
Open fractures are more serious than closed fractures.1 The primary
fracture line is caused by an axial load injury.1 The primary
fracture line goes from anterolateral to posteromedial.1 The primary
fracture line divides the calcaneus into two main fragments: the superomedial
fragment which is also called the constant or sustentacular (SAS) fragment and
the superolateral or tuberosity fragment.1 The superomedial fragment
includes the sustentaculum tali and is stabilized to the talus by ligaments.
So, the talus is attached to the constant fragment.1 The sustentacular
fragment is a useful reference point for fracture reduction.2 The
flexor hallucis longus tendon lies underneath the sustentaculum. If screw
placement to the sustentacular fragment is too long, the flexor hallucis longus
tendon could be affected, causing fixed flexion of the big toe.3
The
Essex-Lopresti classification system is a useful way to differentiate between
different joint fractures. There are two types of Essex-Lopresti fractures: a
tongue-type fracture and a joint depression type fracture.1 In the
tongue-type, the posterior facet is attached to the tuberosity. In the joint
depression type, the posterior facet is not attached to the tuberosity.4
In the tongue-type, the primary fracture line exits anterolaterally and
posteromedially.5 The secondary fracture line appears beneath the
posterior facet and exits posteriorly through the tuberosity.5 The
superolateral fragment and posterior facet are attached to the tuberosity. The
tongue-type fracture can be treated with open reduction and internal fixation.6
In
the joint depression type, the primary fracture line splits the calcaneus
obliquely through the posterior facet and exits anterolaterally and
posteromedially.1 The secondary fracture line exits superiorly just
behind the posterior facet.1 The posterior facet is a free fragment.
The lateral portion of the posterior facet is usually involved and depressed.4
The Sander’s classification of calcaneal fractures is
used to guide the treatment and predict the outcome of the treatment. This
classification system is based on the number of posterior facet fracture
fragments seen on a coronal CT scan.7 Type I is a nondisplaced
fracture which requires nonoperative treatment.7 Type II is a
two-part fracture of the posterior facet.7 Type III is a three-part
fracture of the posterior facet.7 Type II and III calcaneal
fractures benefit from surgery of reduction and fixation.1 Type III
fractures normally result in more arthritis because it has more fracture
fragments and may end by fusion.8 Type IV fractures are highly
comminuted.9 They may require primary subtalar arthrodesis.1
Calcaneal avulsion fractures are typically serious. These
types of fractures require urgent reduction and internal fixation to prevent
skin complications.10 In joint depression fractures of the
calcaneus, the swelling must go down before surgery. Avulsion fractures of the
calcaneus are emergencies, so emergency surgery is performed before the
swelling goes down. Open reduction and internal fixation of the calcaneus is
generally delayed for 1-2 weeks to allow for improvement of the soft tissue
swelling, except with avulsion fractures.1 Avulsion fractures can
cause skin tenting and urgent reduction is recommended.10
There are many associated conditions with calcaneal
fractures. Ten percent are associated with spinal fractures.11 Ten
percent are associated with compartment syndrome of the foot.12 If
this is neglected, it will lead to claw toes due to contracture of the
intrinsic flexor muscles.12 Approximately ten percent are associated
with bilateral fractures.13 Sixty percent are associated with
calcaneocuboid joint fractures.14 Calcaneal fractures may also be
associated with peroneal tendon subluxation. Peroneal tendon subluxation may be
detected on axial CT scans or it may be seen as an avulsion fracture of the
fibula on x-rays.15
Complication
rates for calcaneal fractures are high. Factors associated with poor outcomes are
age greater than 50, smoking, early surgery, history of a fall, heavy manual
labor, males, bilateral injury, workman’s compensation, and peripheral vascular
disease.1,16,17 Men do worse with calcaneal fractures than women.
Calcaneal fractures in men are normally associated with workman’s compensation,
heavy labor, and a 0˚ Bohler angle.1 These fractures typically need
subtalar fusion.18 Calcaneal fractures in females have a simple
fracture pattern. Since calcaneal fractures in males are usually more severe,
it follows that better outcomes are seen in females with calcaneal fractures.19
The
Bohler angle is measured on lateral x-rays.1 This angle is normally
between 20˚-40˚.1 The Bohler angle is formed by a line drawn from
the highest point of the anterior process of the calcaneus to the highest point
of the posterior facet and a line drawn tangential to the superior edge of the
tuberosity.1 A decrease in this angle indicates a collapse of the
posterior facet.1 When viewing calcaneal fractures with the Harris
view, the calcaneus appears to be shortened and widened with varus.1
When viewing calcaneal fractures through CT scans, the axial cut shows the
calcaneocuboid joint and peroneal tendon subluxation.1,20 The
sagittal view shows the subtalar joint and its depression.21 The
coronal view shows the displacement of the posterior facet.22
Coronal CT scans can also show the number of the joint fracture fragments.1
The surgical outcome of calcaneal fractures correlate with the number of the
joint fracture fragments and the quality of reduction.1 MR imaging shows
stress fractures of the calcaneus and the integrity of the peroneal tendons.23,24
Stress fractures of the calcaneus may be misdiagnosed as
plantar fasciitis.25 Stress fractures usually occur in female
runners.26 It is characterized by swelling and tenderness with
medial and lateral compression of the hindfoot during the squeeze test.27 If
the X-ray is negative, an MRI should be obtained. The fracture will be seen in
T1 MR imaging as a linear streak or a band of low signal intensity in the
posterior calcaneal tuberosity.28 In T2 imaging, the signal will be
increased.28
There
are several complications with calcaneal fractures. Wound-related complications
are the most common complication.29 Wound-related complications
occur more in smokers, diabetics, and patients with open fractures.1
Open fractures of the calcaneus is another common complication. Open fractures
of the calcaneus can lead to amputation.30 There is also a high risk
of infection with open fractures.30 Grade I and Grade II open
fractures have wounds that open medially. Open reduction and internal fixation
(ORIF) can be done to treat this complication.30 Open reduction and
internal fixation should not be done in Grade III medial wounds and in most
lateral wounds.30 Another complication is malunion of the calcaneus.31
This is characterized by widening of the heel, varus deformity, and loss
of height.31 The talus is dorsiflexed, limiting dorsiflexion of the
ankle.31 Peroneal tendon irritation and impingement from the lateral
wall is another complication.32
Surgery
on the calcaneus decreases the risk of post-traumatic arthritis.33 Tongue-type
and joint depression type fractures may benefit from open reduction and
internal fixation.6 Subtalar distraction arthrodesis is a good
operation to treat calcaneal fractures associated with loss of height and
limited dorsiflexion of the ankle.31 This operation improves talar
inclination and decreases anterior ankle impingement.31
Additionally, it takes care of arthritis in the subtalar joint.31
Another surgical approach is extensile lateral approach. The lateral calcaneal
artery provides blood supply to the lateral flap associated with the calcaneal
extensile approach.34 It is important to be aware that the Sural
nerve is in the vicinity of the surgical area.35 Delayed wound
healing is a common complication in the extensile lateral approach.35
References:
1. Trompeter A, Razik A, Harris M. Calcaneal fractures:
Where are we now? Strategies in Trauma and Limb Reconstruction.
2017;13(1):1–11.
2. Berberian W, Sood A, Karanfilian B, Najarian R, Lin S,
Liporace F. Displacement of the SUSTENTACULAR fragment in INTRA-ARTICULAR
CALCANEAL FRACTURES. Journal of Bone and Joint Surgery. 2013;95(11):995–1000.
3. Carr JB. Complications of CALCANEUS fractures
entrapment of the Flexor hallucis longus. Journal of Orthopaedic Trauma.
1990;4(2):166–8.
5. White EA, Skalski MR, Matcuk GR, Heckmann N, Tomasian
A, Gross JS, et al. Intra-articular tongue-type fractures of the calcaneus:
Anatomy, injury patterns, and an approach to management. Emergency Radiology.
2018;26(1):67–74.
6. Chhabra N, Sherman SC, Szatkowski JP. Tongue-type
calcaneus fractures: a threat to skin. The American Journal of Emergency
Medicine. 2013;31(7).
7. Jiménez-Almonte JH, King JD, Luo TD, Aneja A,
Moghadamian E. Classifications in Brief: Sanders classification OF
INTRAARTICULAR fractures of the calcaneus. Clinical Orthopaedics & Related
Research. 2018;477(2):467–71.
8. Rammelt S, Marx C. Managing severely malunited
calcaneal fractures and fracture-dislocations. Foot and Ankle Clinics.
2020;25(2):239–56.
9. Piovesana LG, Lopes HC, Pacca DM, Ninomiya AF, Dinato
MC, Pagnano RG. Assessment of reproducibility of sanders classification for
calcaneal fractures. Acta Ortopédica Brasileira. 2016;24(2):90–3.
10. Berringer R. Avulsion fracture of the calcaneus.
Canadian Medical Association Journal. 2018;190(45).
11. Rowe CR. Fractures of the os calcis. JAMA.
1963;184(12):920.
12. Myerson Mark, Manoli Arthur. Compartment syndromes of
the foot after calcaneal fractures. Clinical Orthopaedics and Related Research.
1993;&NA;(290).
13. Popelka V.
Súčasné trendy v liečbe intraartikulárnych zlomenín pätovej kosti [Current
Concepts in the Treatment of Intra-Articular Calcaneal Fractures]. Acta Chir
Orthop Traumatol Cech. 2019;86(1):58-64. Slovak. PMID: 30843515.14.
14. Kinner B, Schieder S, Müller F, Pannek A, Roll C.
Calcaneocuboid joint involvement IN CALCANEAL FRACTURES. Journal of Trauma:
Injury, Infection & Critical Care. 2010;68(5):1192–9.
15. Park C-H, Gwak H-C, Kim J-H, Lee C-R, Kim D-H, Park
C-S. Peroneal tendon Subluxation and dislocation In CALCANEUS FRACTURES. The
Journal of Foot and Ankle Surgery. 2021;60(2):233–6.
16. Su J, Cao X. Can operations achieve good outcomes in
elderly patients with SANDERS II–III calcaneal fractures? Medicine.
2017;96(29).
17. Clare MP, Crawford WS. Managing complications of
CALCANEUS FRACTURES. Foot and Ankle Clinics. 2017;22(1):105–16.
18. Csizy M, Buckley R, Tough S, Leighton R, Smith J,
McCormack R, et al. Displaced Intra-articular CALCANEAL FRACTURES. Journal of
Orthopaedic Trauma. 2003;17(2):106–12.
20. Toussaint RJ, Lin D, Ehrlichman LK, Ellington JK,
Strasser N, Kwon JY. Peroneal tendon DISPLACEMENT Accompanying INTRA-ARTICULAR
CALCANEAL FRACTURES. Journal of Bone and Joint Surgery. 2014;96(4):310–5.
21. Badillo K, Pacheco JA, Padua SO, Gomez AA, Colon E,
Vidal JA. Multidetector CT evaluation Of CALCANEAL FRACTURES. RadioGraphics.
2011;31(1):81–92.
22. Buckley R. Displaced fracture of the calcaneus body
[Internet]. AO Foundation Surgery Reference. [cited 2021Sep29]. Available from:
https://surgeryreference.aofoundation.org/orthopedic-trauma/adult-trauma/calcaneous/displaced-body-fractures/definition
23. Kato M, Warashina H, Kataoka A, Ando T, Mitamura S.
Calcaneal insufficiency fractures following ipsilateral total knee
arthroplasty. Injury. 2021;52(7):1978–84.
24. Park HJ, Cha SD, Kim HS, Chung ST, Park NH, Yoo JH,
et al. Reliability of MRI findings OF PERONEAL Tendinopathy in patients with
LATERAL CHRONIC Ankle Instability. Clinics in Orthopedic Surgery.
2010Nov5;2(4):237.
25. Weber JM, Vidt LG, Gehl RS, Montgomery T. Calcaneal
stress fractures. Clinics in Podiatric Medicine and Surgery. 2005;22(1):45–54.
26. Labronici P, Pires RE, Amorim L. Calcaneal stress
fractures in civilian patients. Journal of the Foot & Ankle.
2021;15(1):54–9.
27. Kiel J,
Kaiser K. Stress Reaction and Fractures. 2021 Aug 4. In: StatPearls [Internet].
Treasure Island (FL): StatPearls Publishing; 2021 Jan–. PMID: 29939612.
28. Lawrence DA, Rolen MF, Morshed KA, Moukaddam H. MRI of
heel pain. American Journal of Roentgenology. 2013Apr18;200(4):845–55.
29. Ding L, He Z, Xiao H, Chai L, Xue F. Risk factors for
postoperative wound complications of calcaneal fractures following plate
fixation. Foot & Ankle International. 2013;34(9):1238–44.
30. Heier KA, Infante AF, Walling AK, Sanders RW. Open
fractures of THE Calcaneus: Soft-tissue Injury DETERMINES OUTCOME. The Journal
of Bone and Joint Surgery-American Volume. 2004;86(11):2569.
31. Guang-Rong Y, Xiao Y. Surgical management Of
Calcaneal Malunion. Journal of Orthopaedics, Trauma and Rehabilitation.
2013;17(1):2–8.
32. Davis D,
Seaman TJ, Newton EJ. Calcaneus Fractures. 2021 Aug 9. In: StatPearls
[Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan–. PMID:
28613611.
33. Vilá-Rico J, Ojeda-Thies C, Mellado-Romero MÁ,
Sánchez-Morata EJ, Ramos-Pascua LR. Arthroscopic posterior subtalar arthrodesis
for salvage of posttraumatic arthritis following calcaneal fractures. Injury.
2018;49.
34. Mehta CR, An VV, Phan K, Sivakumar B, Kanawati AJ,
Suthersan M. Extensile lateral versus sinus Tarsi approach For displaced,
intra-articular Calcaneal Fractures: A meta-analysis. Journal of Orthopaedic
Surgery and Research. 2018;13(1).
35. Buckley R. Extended lateral approach to the calcaneus
[Internet]. AO Foundation Surgery Reference. [cited 2021Sep29]. Available from:
https://surgeryreference.aofoundation.org/orthopedic-trauma/adult-trauma/calcaneous/approach/extended-lateral-approach-to-the-calcaneus
Fractures of the olecranon may occur due to a direct blow to
the elbow or from a fall onto an outstretched hand. Nondisplaced fractures have
less than 2mm of separation and are considered stable. Fracture separation will
not increase with elbow flexion. Extensor mechanism is intact and the patient
will be able to extend the elbow against gravity. Displaced fractures could be
an avulsion, oblique, transverse, comminuted, or dislocated.
Olecranon fracture dislocations can be anterior (transolecranon)
or posterior (similar to monteggia fracture dislocation). An examination will
show that the patient is unable to extend the elbow with these displaced
fracture types. A true lateral view x-ray will clearly show the olecranon
fracture. Usually, these fractures are followed by stiffness of the elbow in
about 50% of the patients. However, this does not affect the function.
The goal of treatment for olecranon fractures should be
restoration of the articular surface, preservation of the continuity of
extensor mechanisms, maintain elbow stability, and avoid stiffness of the
elbow. Nonoperative treatment is used for nondisplaced fractures and it may be
used for some displaced fractures in elderly patients (treat elbow in some
flexion with a splint). I would personally use minimally invasive techniques in
these patients unless the skin is very bad, or the fracture is very comminuted.
There are three techniques used for surgical treatment: the
tension band technique, detach olecranon and reattach triceps, and plate and
screw fixation. The tension band technique is only used for transverse fractures
with no comminution. K-wires and screws are used, and the surgeon may use
either a 6.5mm screw or Kwires for the tension band. When doing the tension
band technique, you want to engage the anterior cortex of the ulna. The surgeon
should avoid over penetration to avoid affecting the forearm rotation or
injuring the anterior interosseous nerve. The surgeon needs to be sure that the
pins are not fixing the radius and that after the operation, the patient can
perform pronation and supination of the forearm (pull the pins out slightly if
needed). The distractive force of the triceps is converted to compression force
at the articular surgace, especially when bending the elbow. The drill hole for
the K-wire should be positioned about 4-5cm from the fracture which gives
enough safe distance so that the fracture will not propagate. Place the tension
band wire through the drilled holes before application of the K wires. The
surgeon should be sure that the hook to the K-wire is posterior. Make sure that
the tension band wire is close to the bone so there is no laxity in the
fixation and instability. An intramedullary screw could be used. This screw
fixation may need a washer to capture the tension band wire. Intramedullary
6.5mm screw fixation is a reasonable option for fixation but it may need to be supplemented
with tension band wires. Never use cancellous screw alone. The tension band
technique are for transverse fractures of the olecranon. If fractures
comminution is present, change the plan of fixation.
When detaching the olecranon and reattaching the triceps, an
excision of the fracture fragment and triceps advancement is used:
If the fracture is less than 50%
To treat elderly patients (especially if
fracture is comminuted)
For some nonunions when the fracture is small
and cannot be fixed
The surgeon must be sure that the procedure is done with the
elbow is stable. If the elbow has ligamentous instability and excision of the
fracture fragment is done, this will make the elbow very unstable. The triceps
should be attached closer to the articular surface.
Special olecranon plates are available when using a plate
and screw fixation technique. The bridge plate and screw fixation technique is
used in comminuted, Monteggia, oblique fractures extending to the coranoid, and
fracture dislocation. The plate is placed on the tension side of the olecranon
(dorsal side). Sometimes, an opening is made through the triceps and the plate
is placed against the bone, then suturing the triceps tendon over the plate to
avoid hardware prominence.
In summary, if the patient is elderly with a small,
comminuted fracture fragment less than 50% of the joint space, excise the
fragment, and reattach the triceps tendon to the olecranon. If the olecranon
fracture is transverse and proximal to the base of the coranoid process, then
use the tension band technique. Use plate fixation for all olecranon fracture
scenerios, such comminuted fractures, oblique fractures, unstable fractures, dislocation,
or fractures distal to the coranoid process. The typical exam question scenario
will discuss a comminuted fracture that should be treated with a plate. You
probably need to remove above 20% of the plate fixations due to hardware irritation.
Hardware irritation is worse with the tension band surgical treatment (may need
to remove in more than 50% of cases).
A patient with a complete anterior interosseous nerve injury
or a high medial nerve injury should be asked to make a fist. The first and
second digits will have difficulty in flexing, while the other digits will
flex. The third digit will be weak, while the fourth and fifth digits are
normal. This position of the hand is similar to the position taken during a
hand blessing. The Benedictine sign is different from an “ulnar claw hand”.
Ulnar claw hand refers to damage to the ULNAR nerve and is seen when attempting
to extend all the digits (leaving the 4th and 5th digits
flexed). The O.K. sign is used to check for paralysis of the anterior
interosseous nerve due to entrapment or compression injury. A patient with
paralysis of the anterior interosseous nerve will be unable to make the O.K.
sign. This is due to weakness of the flexor pollicis longus and flexor
digitorum profundus muscles. A typical pinch attitude is associated with
anterior interosseous nerve injury.
The anterior interosseous nerve arises from the median nerve
about 4-6cm distal to the elbow, which is about 1/3 of the way down the
forearm. It exits from the anterolateral aspect of the median nerve and it runs
between the radius and the ulna on the interosseous membrane between and below
the muscles of the flexor digitorum profundus and the flexor pollicis longus.
The anterior interosseous nerve supplies the flexor digitorum profundus muscle
for the index and long fingers. It also supplies the flexor pollicis longus and
the pronator quadratus muscles. The flexor digitorum profundus muscle for the
index and long fingers is supplied by the anterior interosseous nerve. The
medial part of the FDP is supplied by the ulnar nerve (FDP has dual
innervation). The anterior interosseous nerve passes dorsal to the pronator
quadratus with the anterior interosseous artery and provides innervation to the
volar wrist capsule. The terminal branch of the anterior interosseous nerve
innervates the carpal joint capsule.
In patients with Martin-Gruber Connection, the median nerve,
or anterior interosseous nerve to the ulnar nerve in the forearm may present
with intrinsic muscle weakness. It may be differentiated also from
Parsonage-Turner Synrome (acute brachial plexus neuritis) and patient may have
pain in the affected extremity. In anterior interosseous nerve entrapment, the
median nerve conduction study result will be normal, however the needle EMG of
the anterior interosseous innervated muscles will be abnormal.
There are some important tests that every Orthopaedic
Surgeon should think about. This doesn’t mean the tests are needed for every
patient. It just means that the physician needs to think about these tests to
see if it will benefit the patient or not. Some tests commonly ordered are
hemoglobin A1C (HbA1c), Vitamin D25, and C-reactive protein (CRP) &
sedimentation rate.
Hemoglobin A1C test are ordered for diabetic patients. HbA1c
is a good test for monitoring long-term glucose (sugar) control on patients with
diabetes. HbA1c is a percentage of the glycanated hemoglobin relative to the total
hemoglobin in the blood. The normal range of HbA1c is 4-6%. More than 7% is
high. Another test, the 25-Hydroxy Vitamin D blood test is ordered for patients
with osteoporosis, nonunions, fragility fractures, and occasionally in patients
with infections. If infection is suspected and the physician needs to monitor
the progress of treatment, C-reactive protein (CRP) & sedimentation rate
tests should be ordered. A Methicillin-resistant staphylococcus aureus (MRSA)
screening should be ordered for patients who could be carriers. Nutritional
assessments may be necessary for other patients.
Joints should be aspirated prior to injecting of the joint.
The physician should additionally be sure that there is no infection when
injecting the joint. A fluid analysis from the joint should be completed.
Important vascular studies that can be ordered include: A.B.I., CTA, or a
Doppler. Some radiological studies are performed with a dye injection. For
example, an MRI of the spine will require gadolinium, while an MRI arthrogram
may be used for the hip or shoulder. Tests rarely ordered include: alpha-defensin
test (infection); Nicotine/Cotinine test (smoking); Protein S, Protein C, or
Factor 5 leiden tests. There are some special tests and precautions that must
be taken for patients with epilepsy. It is important that the physician does
not perform a procedure if the epilepsy is not controlled. It is important to
know that anti-epileptic medication can interfere with vitamin D metabolism in
the liver.
Patients on anticoagulation medications should be monitored,
especially patients with atrial fibrillation, which makes the orthopaedic
procedure more complicated. You want to give the patient anticoagulation, but
not encroaching on the management of atrial fibrillation. Patients with a short
or thick neck, or a history of sleep apnea, may need additional sleep studies before
surgery and may need special precautions after surgery. Sleep apnea will affect
the post-operative care of the patient. The physician should avoid ordering unnecessary
tests and focus on ordering the most important tests. Orthopaedics deal with
concepts and every condition will have a reasonable way of diagnosing it and a
reasonable way of treating it.
Adhesive Capsulitis, or frozen shoulder, is a painful progressive
loss of shoulder motion. It affects both active and passive movement of the
shoulder joint. The shoulder will be stiff and painful and occurs due to
inflammation, fibrosis, scarring, and contraction of the capsule. A normal
shoulder joint capsule is elastic and allows great range of motion.
Inflammation and thickening of the shoulder capsule and may lead to adhesive
capsulitis. Frozen shoulder may occur without any specific cause, however it
may be triggered by a mild trauma to the shoulder.
This condition develops slowly and goes through three
phases:
Pain and freezing
Stiffness or frozen
Resolution
During the pain and freezing phase, the pain is worse at
night and increases with any movement. This phase will last several months.
During the second phase, range of motion is limited as pain is diminishing.
This may last up to one year. The resolution phase may begin overtime and may
last up to three years.
Conditions associated with frozen shoulder include:
Diabetes
Thyroid problems
Auto immune disease
Stroke
Rheumatoid arthritis
Trauma or post-surgery
A patient with frozen shoulder will have loss of both active
(movement without assistance) and passive (movement with assistance) motion.
External rotation of the shoulder is very limited and the condition is
self-limiting and may resolve on its own. X-rays are needed to rule out
degenerative arthritis. An MRI or
arthrogram will show small fluid in joint cavity. Rotator cuff may be normal
and synovitis and narrowing of the rotator cuff interval is usually seen.
Treatment consists of anti-inflammatory medications,
physical therapy, injections, and manipulation under anesthesia. Surgery will
be done in the form of a release of the capsule when nonoperative methods fail.
The physician should always check the patient for diabetes.
The posterior cutaneous nerve of the thigh (small sciatic
nerve) arises from the sacral plexus from S1-S3. The posterior cutaneous nerve
of the thigh exits from the pelvis through the greater sciatic notch below the
piriformis muscle. The nerve descends below the gluteus maximus muscle along
with the inferior gluteal artery. It runs into the back of the thigh beneath
the fascia lata and over the long head of the biceps femoris muscle to the back
of the knee. The nerve then pierces the deep fascia and accompanies the short
saphenous vein to the middle of the back of the leg. The posterior cutaneous
nerve of the thigh innervates the distal part of the gluteal region, the skin
of the perineum and the posterior part of the thigh.
The nerve can become compressed
when passing through the tunnel below the piriformis muscle and under the
gluteus maximus muscle. This may result in sensitivity disturbances of the
innervation area of the nerve. Causes of the syndrome may be hypertrophy or
abnormality of the piriformis muscle such as entrapment below the piriformis
which compresses the nerve. Compression of the nerve can also occur due to
prolonged sitting. During the clinical examination, pain and sensitivity will
be evident. Pain and sensitivity disturbances are characteristic of the nerve
distribution site in the posterior part of the thigh down the knee. This
disturbance can be from hyperesthesia to hypoesthesia or burning sensation
similar to meralgia paresthetica of the lateral cutaneous nerve of the thigh.
Differential diagnosis include piriformis syndrome. The
patient should avoid sitting for long periods of time, especially on a hard
base. Treatment consists of physical therapy, massage, and injection. Surgery
is rarely needed.
A SLAP tear is a tear that occurs where the biceps tendon
inserts into the superior labrum. A SLAP tear is different from a Bankart
lesion. SLAP tears are not common and can be hard to diagnose. Symptoms of a
SLAP tear include: pain deep within the shoulder or in the back of the
shoulder, as well as catching, popping, or clicking sensations. The patient may
also experience pain when throwing a ball with a decrease in velocity and the
feeling of having a dead arm after pitching. Patients will also experience pain
with overhead activity which mimics impingement syndrome. This typically
affects throwing athletes. When the biceps tendon is involved, pain may also be
located at the front of the shoulder. A SLAP tear can be an isolated lesion or
it can be associated with internal impingement, articular sided cuff tear, or
instability.
A SLAP tear is diagnosed with a clinical examination and
testing. The O’Brien’s test is the most commonly used test. Multiple tests are
usually used including the anterior slide test and the clunk test. An MRI with
contrast is the best imaging technique. When performing the O’Brien’s test, the
patient is standing or sitting with the arm at 90° of flexion, 10° of
adduction, and full internal rotation with the forearm pronated. The examiner applies pressure to the forearm
and instructs the patient to resist the applied downward force. Pain at the
shoulder joint suggests a SLAP lesion. Decrease in pain of the shoulder joint
on supination of the arm is suggestive of a SLAP tear.
Treatment consists of physical therapy, anti-inflammatory
medications, injections, and surgery (when conservative treatment fails). If
surgery is necessary, a labral debridement will be performed for minor tearing
and fraying. Biceps Tenodesis is becoming popular, as it is a procedure that
cuts the biceps tendon where it attaches to the labrum and reinserts it in
another area, usually in front of the shoulder. A biceps tenotomy is a
procedure that cuts the biceps tendon from the glenoid, releasing the long head
of the biceps tendon from its attachment allowing it to fall into the upper arm
out of the shoulder joint. A biceps tenotomy is probably best suitable for some
elderly patients. A SLAP repair is a procedure which uses sutures to anchor the
torn labrum to the glenoid. This repair is usually done for athletes and
patients under the age of 40 years.
To view my Youtube video, 'Massive Rotator Cuff Tear- Classic', click here.
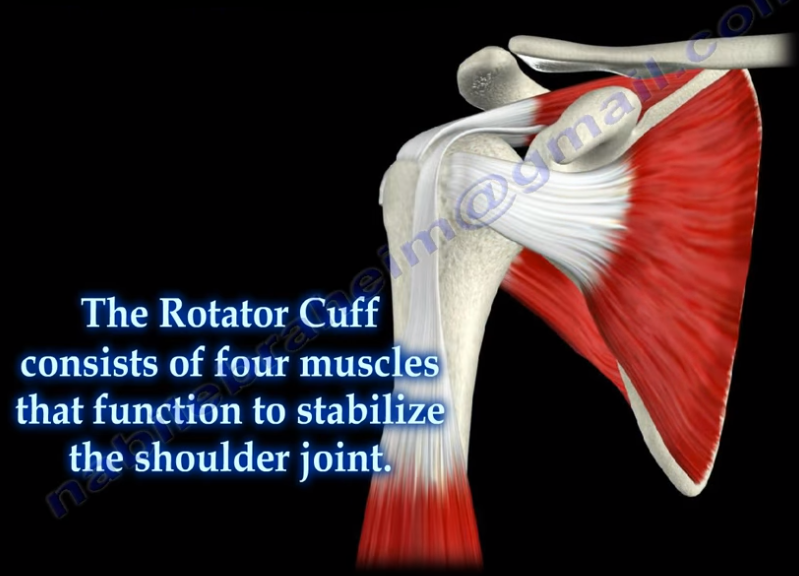
Massive rotator cuff tears are a disabling problem. These
tears can cause pain, weakness, and sometimes swelling of the shoulder. The
rotator cuff consists of four muscles that function to stabilize the shoulder
joint: supraspinatus rotator cuff tendon, subscapularis tendon, infraspinatus
rotator cuff tendon, and the teres minor rotator cuff tendon. The supraspinatus
tendon is the most common of the rotator cuff tendons to become ruptured. Massive
tears of the rotator cuff that are greater than 5cm usually involving both the
supraspinatus and infraspinatus tendons.
Massive tears of the rotator cuff are defined as tears
greater than 5cm, usually involving both the supraspinatus and infraspinatus
tendons. Retraction of the rotator cuff tendons along with muscle atrophy and
fatty infiltration can occur. This makes surgical reconstruction difficult with
the surgical outcome being unpredictable and less than satisfactory.
Treatment varies from physiotherapy to replacement of the
humeral head. Arthroscopic or open repair is usually the selected treatment.
Reconstruction can be done in selected cases. A rotator cuff arthropathy is
performed on massive cuff tears that are associated with superior migration of
the humeral head as well as instability and arthritis of the shoulder. The
patient will have pseudoparalysis and an x-ray will show shift of the humerus
proximally. An MRI will show massive cuff tear with retraction at the level of
the glenoid with atrophy of the muscle and fatty infiltration. A reverse shoulder
is the treatment of choice for the elderly with rotator cuff arthropathy as it
improves the pain and function. Hemiarthroplasty is the treatment for younger
patients. A standard head or a big humeral head can be selected.
A patient with a massive tear of the cuff usually develops
weakness of the shoulder and becomes unable to actively lift the arm without
assistance. Fluid collection within the shoulder may occur with a massive tear
of the rotator cuff.