
Wednesday, November 16, 2016
Thursday, November 10, 2016
Bone Remodeling in Children
Children have a unique ability for healing of their fractures
and remodeling of their deformities. The physician should strive to achieve
anatomic reduction of fractures in children.

The surgeon may not be able to achieve acceptable reduction every
time, fractures do not always remodel. The deformity may lead to unacceptable
results in cosmesis and function.
What are the rules for remodeling in children?
Age of the patient:
Younger children have better remodeling potential. The
younger, the better. Children with two or more years of growth left have a
chance for remodeling. The periosteum in children is thick and promotes faster
healing of the fracture as well as increased potential for remodeling.
Distance:
The distance of the fracture from the end of the bone.
Fracture in the metaphysis remodels better than in the middle of the bone. A fracture
in the middle of the bone has less potential for remodeling.
Severity of
Angulation
If there is minimal angulation, the bone could remodel
completely. Where angulation is more severe, the bone will partially remodel.
Angulation in the plane of joint movement is most likely to improve with growth
and remodeling.
Remodeling will not improve displaced fractures involving
the joint or the growth plate.
Wednesday, November 2, 2016

Back Pain
There
is certain etiology of low back pain in 85% of cases. Patients with a single occurrence
of low back pain return to work within 6 weeks 90%of the time. Moreover, most
patients get better with time. In fact, about 60% of patients get better in approximately
10 days.

Low
back pain is the second most common cause of work absenteeism. If a person has
a history of low back pain, it is likely they could develop occupational low
back pain. Persistent back pain for more than 6 months constitutes only four
percent of cases. Disability is usually closely related to compensation and
litigation.
The
least amount of pressure on the discs is measured with the patient lying in the
supine position. The highest amount of disc pressure is measured while sitting
with 20 degrees of forward leaning with a 20 kg load in the arms. It is better
to keep the weight of the load close to the body. This will reduce the
compressive forces placed on the lumbar spine. Yoga activities and exercises
performed during sitting probably have less pressure being placed on the discs.
Physical
factors which lead to low back pain include the following: lack of fitness;
heavy lifting of objects; operating motor vehicles; prolonged sitting;
operating motor vehicle accidents; prolonged sitting; operating vibrating
tools; and cigarette smoking (nicotine causes disc degeneration).
There
are many sports-related activities related to low back pain. When golfing, pain
occurs as the result of twisting, bad forward bending, and most importantly
overarching the spine during the swing. After the age of 40, we lose about 50%
of our rotational spine movement. It is important to stretch and warm-up before
starting the game. Vibration caused by horseback riding increases the load on
the discs. The back muscles work constantly to keep posture straight. Caring
for horses could also be detrimental to the back due to the bending and lifting
associated with their care.
Virtually
any structure in the spine can hurt including: the facet Joints; invertebral
discs; spinal canal; sacroiliac joints; muscles; ligaments; nerves; hip joints/Piriformis
muscles; and trochanteric bursitis. Red flags for cancer include: over 50 years
of age; pain at rest and night; unexplained weight loss; history of cancer; and
bone destruction involving the pedicle is pathognomonic. Red flags for
infection include: diabetes; fever; drug abuse; urinary tract infection; and
previous surgery
Treatment
for acute low back pain, without sciatica (leg pain), involves a short period
of bed rest, anti-inflammatory medications, and physical therapy for a short
period of time. Patients will also be advised to work within the limits of
pain.
Tuesday, November 1, 2016
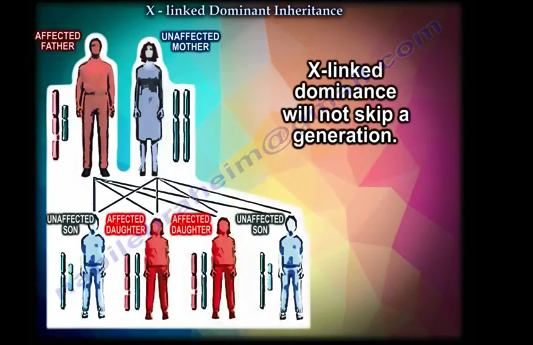
X Linked Dominant Inheritance
Some orthopaedic conditions that Dr. Nabil Ebraheim has seen throughout his years as a surgeon are caused by genes.
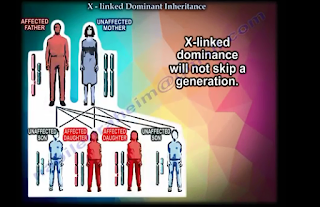 X-linked dominance will not skip a generation.
X-linked dominance will not skip a generation.
One example of an x-linked dominant issue is Leri-Weill Dyschondrosteosis (LWD). LWD is a dominantly inherited skeletal dysplasia characterized by short stature, mesomelia, and Madelung wrist deformity. This is a rare genetic disorder caused by a mutation of the SHOX gene. The shortened stature is caused by the homeobox containing gene.
Hypophosphatemic Rickets is a vitamin D resistant rickets. X-linked hypophosphatemic rickets with inability of the renal tubules to absorb phosphates (phosphates levels are down linked to the PHEX gene - Phosphate Regulating Endopeptidase Homolog, X-linked). This is the most common cause of rickets within the United States of America. Dr. Nabil Ebraheim suggests that the doctor will look for a child short in stature, bowing of the lower limbs, and low serum phosphate levels. The Alkaline phosphatase (ALP) levels will also be high. Calcium levels in these patients will be normal, as well as the Parathyroid hormone (PTH). The treatment for this is usually high doses of phosphate replacement and high doses of vitamin D to facilitate the phosphate absorption.
In x-linked dominance, the affected individual has an affected parent due to the dominant gene. All affected males must have an affected mother. All affected fathers will have affected daughters and no affected sons. Dr. Nabil Ebraheim suggests looking to the males. Looking and the sons and fathers will be your clues.
Dr. Nabil Ebraheim's YouTube Channel
Dr. Ebraheim's Huffington Post
One example of an x-linked dominant issue is Leri-Weill Dyschondrosteosis (LWD). LWD is a dominantly inherited skeletal dysplasia characterized by short stature, mesomelia, and Madelung wrist deformity. This is a rare genetic disorder caused by a mutation of the SHOX gene. The shortened stature is caused by the homeobox containing gene.
Hypophosphatemic Rickets is a vitamin D resistant rickets. X-linked hypophosphatemic rickets with inability of the renal tubules to absorb phosphates (phosphates levels are down linked to the PHEX gene - Phosphate Regulating Endopeptidase Homolog, X-linked). This is the most common cause of rickets within the United States of America. Dr. Nabil Ebraheim suggests that the doctor will look for a child short in stature, bowing of the lower limbs, and low serum phosphate levels. The Alkaline phosphatase (ALP) levels will also be high. Calcium levels in these patients will be normal, as well as the Parathyroid hormone (PTH). The treatment for this is usually high doses of phosphate replacement and high doses of vitamin D to facilitate the phosphate absorption.
In x-linked dominance, the affected individual has an affected parent due to the dominant gene. All affected males must have an affected mother. All affected fathers will have affected daughters and no affected sons. Dr. Nabil Ebraheim suggests looking to the males. Looking and the sons and fathers will be your clues.
Dr. Nabil Ebraheim's YouTube Channel
Dr. Ebraheim's Huffington Post
Monday, October 31, 2016
AO/ASIF Foundation
Prior to becoming the Trauma Fellowship Program Director and Orthopaedic Residency Program Director at the University of Toledo Medical Center, Dr. Nabil Ebraheim completed an AO Fellowship (technique of internal fixation) at Kantonsspital Chur in Switzerland. Possessing particular experience in handling spinal fusions and bone fractures, Dr. Nabil Ebraheim is considered a leading expert in the field of orthopedics.
Established in Switzerland in 1958, the AO technique of internal fixation, also known as the Association of the Study of Internal Fixation (ASIF) set out to change the way fracture treatments were performed. The association developed revolutionary instruments for use in treatment procedures along with advanced implants to help with recovery.
The AO/ASIF Foundation included 90 of the world’s leading trauma surgeons, and it created more teaching and training opportunities for these experts to promote their research. The clinical documentation and trauma treatment taught by the organization is responsible for many modern advancements in the field of orthopedics.
Wednesday, October 5, 2016


Subscribe to:
Posts (Atom)