Measles, also known as Rubeola, is an extremely contagious
viral infection caused by a Paramyxovirus. It usually occurs in children under
the age of 5 years and the reservoir for this virus is the human respiratory
tract. Transmission occurs through inhalation of infected droplets produced by
infected individuals by sneezing, coughing, or even talking.
Risk factors to contracting this viral infection include:
Lack of vaccination
Travelling to endemic areas
Vitamin A deficiency
Immunocompromised individuals
The measles virus has an incubation period of 10-14 days
during which the patient has no signs or symptoms. After the 14 days of the
incubation period, the patient will start developing the following signs and
symptoms—fever, cough, coryza (runny nose), and conjunctivitis (pink eye). A characteristic rash also develops which is a
red maculopapular rash appearing first on the face- behind the ears, and then
spreads downwards towards the neck, trunk, arms, legs, and feet. Disease specific
Koplik Spots may develop, which are tiny white spots that appear on the buccal
mucosa.
A measles patient is infective for a total duration of 8
days. Infectivity starts four days before the appearance of the rash and stops
around the fourth day of having the rash. Thus, the patient may appear to be
well and still infect other people.
A diagnosis is usually achieved by thorough history taking
and examination to identify disease specific features such as the unique rash
patter and the characteristic koplik spots. Blood tests could be ordered to
confirm the presence of measles IgM antibodies. Furthermore, respiratory
specimens may be obtained to isolate the virus.
Complications of Measles include:
Otitis media
Pneumonia
Laryngotracheitis
Subacute sclerosing panencephalitis
Vaccination is quite important and is considered the most
widely used method of prevention. Widespread vaccination leads to herd immunity, which helps to contain the disease and prevent outbreaks. When only a few
individuals are vaccinated, the disease may spread easily through the
population. The measles vaccine is a live attenuated vaccine that is given to
children as part of the MMR (Measles,
Mumps, and Rubella) vaccine. The vaccine is typically administered by the age
of 1 year, followed by a booster dose at the age of 5. The vaccine helps the
individual develop lymphocytes and anti-bodies to attack and eliminate the
virus upon exposure. It is important to remember not to vaccinate
immunocompromised individuals because this is a live attenuated virus vaccine.
Treatment is largely supportive including fluids, fever
reduction, vitamin A, and in some cases, antibiotics may be given to prevent
superinfection.
It is worth noting that a controversy remains regarding the
use of the measles vaccine.
The neurovascular status must be examined in patients with
supracondylar fractures. Avoid treating the patient with a cast that may cause
hyperflexion of the elbow. Bending the elbow too much may affect the brachial
artery. It may not be acceptable to reduce the fracture at 90° of elbow flexion. In
these cases, choose a different alternative to casting, such as pinning (closed
or open technique).
It is important to remember that Volkmann’s ischemic
contracture may occur due to injury to the brachial artery. You have to make
sure that you restore the circulation.
A few scenarios to go over
1.The Patient has good circulation with no radial
pulse (hand perfused)
a.In this case, you would do a closed reduction
and pinning as well as in-patient monitoring for 24-48 hours in order to assess
the circulation of the extremity
2.Cold Cyanotic Hand (no perfusion or you may have
underperfusion)
a.This
may occur before or after attempting reduction
b.The
patient must immediately go to the operating room for closed or open reduction
and pinning (No matter if the hand is underperfused or perfused at all)
c.Monitor
the circulation for anticipation of improvement
d.If
there is no immediate improvement, explore the antecubital fossa in order to
explore the brachial artery
e.Have
the help of a vascular surgeon
f.Assess
the circulation
You want to think of this scenario like a knee dislocation. If you have
pulses or no pulses with a knee dislocation, then you reduce the knee
dislocation. It is the same with supracondylar fractures: pulses or no pulses,
pink or not pink hand, cold cyanotic hand—do closed reduction and pinning. It
is a more urgent condition if there are perfusion problems.
3.Perfusion
Disappears During Reduction or Monitoring
a.If the
perfusion gets worse after reduction of the fracture, then you need to find out
what has happened.
b.You
will need to perform an open exploration and without an arteriogram
4.Circulation
Disappears After Closed Reduction and Pinning
a.Reduction
caused harm to the patient
b.The
pins need to be removed, the fracture needs to be unreduced and check the
circulation.
c.Check
to make sure that the neurovascular bundle does not become trapped in the
fracture gap after closed reduction and pinning.
Open fractures are categorized with the Gustilo-Anderson Classification. A Grade I Injury indicated a clean wound, less than one centimeter long with minimal injuries to the soft tissue and minimal bone comminution. A Grade II injury consists of a moderately contaminated wound greater than one centimeter long with moderate tissue injury and moderate bone comminution. A highly contaminated wound, usually greater than ten centimeters, segmental fractures, farm yard injuries, high velocity gunshot wounds and fractures occurring in a highly contaminated environment regardless of the size of the wound.
Grade III injuries are classified further into A, B, and C. Grade III A is a severe soft tissue injury with a crushing comminuted fracture; soft tissue coverage of bone possible. Grade IIIB consists of a very severe loss of soft tissue cover with poor bone coverage and variable—may be moderate to severe bone comminution. Grade IIIB usually requires a soft tissue reconstructive surgery in the form of local or distant flaps. Grade IIIC fractures consists of a vascular injury requiring repair or amputation. There is a very severe loss of soft tissue cover with moderate to severe bone comminution. Injury of the femoral artery from the posteriorly displaced proximal fragment of a Grade III C open supracondylar fracture of the femur. Grade III C has a high rate of amputation, nonunion and infection.
Hip Infection (Septic Arthritis)
An infection in the hip is a serious disease especially in children. The intraarticular structures will be inflamed and the increased intracapsular pressure will decrease the blood supply to the femoral head. Infection is associated with a high risk of avascular necrosis. The position of the limb in the stage of effusion, flexion, abduction, and external rotation. Complications are severe and much more common in children. Complications include: pathological dislocation, avascular necrosis, osteomyelitis, and pelvic abscesses. Urgent aspiration followed by drainage of the hip joint combined with intravenous antibiotics are the typical treatment for hip infections.
Necrotizing Fasciitis
Necrotizing Fasciitis is an insidiously advancing soft tissue infection characterized by widespread tissue necrosis. The most common causative organism—group A beta—hemolytic streptococcus. There is a high mortality rate with sepsis and renal failure. Amputation and the mortality rate is increased due to a delay in diagnosis. Predisposing factors for necrotizing fasciitis include: trauma, surgery, as well we urogenital and anogenital infections. There are three types of necrotizing fasciitis: Type I—which is Polymicrobial, Type II—which is a Group A beta-hemolytic streptococcus, and Type III—which is gas gangrene-clostridial myonecrosis. Treatment consists of an immediate surgical debridement combined with intravenous antibiotics and hyperbaric oxygen if necessary.
Fracture with Soft Tissue Compromise
Soft tissue compromise associated with fracture blisters, ecchymosis, and severe bruising which indicate a greater degree of deep soft tissue damage. Blood filled fracture blisters are associated with high wound complications. Initial management involves application of a spanning external fixator with the fracture dislocation held in reduction with traction. The definitive management involves replacing the spanning external fixation with a hybrid fixator or plate once the soft tissue edema is resolved and the skin is wrinkled, usually in one to three weeks. Spanning external fixation can often be combined with percutaneous fixation of large articular fragments. A soft tissue compromise is more common with tibial plateau fractures and tibial pilon fractures with diaphyseal extension. A calcaneal avulsion fracture is considered an emergency. Urgent reduction and fixation is mandatory to avoid soft tissue complications. Type I—is a “sleeve” type tuberosity fracture. This pressure will create skin necrosis and significant soft tissue complication.
Dislocations at the knee occur as a result of a violent
trauma. For example, a Posterior Dislocation—the dashboard injury, is the most
common mechanism of injury which includes exaggerated hyperextension of the
knee and dashboard (posteriorly directed force with the knee flexed at 90
degrees). Posterior dislocation is associated with a high incidence of popliteal
artery injury. With an established popliteal artery injury and resultant
ischemia, blood flow must be restored within 6 hours. Posterior tibialis and
dorsalis pedis pulses should be carefully evaluated in any patient with a knee
dislocation. Look for any evidence of ischemia, diminished blood flow, or
compartment syndrome. Incidence of nerve injury range from 14 percent to 35
percent. Be cautious of spontaneously reduced knee dislocations and its
associated pathology.
Urgent reduction of the knee dislocation is mandatory. Once
the reduction is complete, it is important to reevaluate circulation. If the
circulation is normal, serial follow-up up to 48 hours with clinical
examination and non-invasive studies (ABI). If the circulation is abnormal, an
arteriography should be performed. If no pulses are palpable, immediate
exploration will need to be initiated. The arterial injury is treated,
circulation restored, and prophylactic fasciotomy may be necessary.
Posterior Sternoclavicular Joint Dislocation
A Posterior Sternoclavicular Joint Dislocation typically results
from either a direct force applied to the front of the medial clavicle or an
indirect force applied to the posterolateral aspect of the shoulder. Posterior
dislocation of the sternoclavicular joint could be missed. It is imperative to look
for compression of the trachea, esophagus, or great vessels of the neck. A
posterior dislocation is difficult to diagnose by x-ray so a CT scan is the
preferred method for diagnosing the dislocation and any associated
complications. An urgent reduction is mandatory in order to assure that a
closed reduction is successful and stable. Open reduction may be performed if a
closed reduction is unsuccessful. If an open reduction is decided, during the
operation, a cardiac surgeon will be waiting standby.
Scapulothoracic Dissociation
Scapulothoracic Dissociation is a rare entity that consists
of disruption of the scapula-thoracic articulation. It is a closed avulsion of
the scapula with associated clavicular fracture or disruption of its
articulations and severe soft tissue injury. This injury has been described as
a closed, traumatic fore-quarter amputation. It is a traumatic lateral
displacement of the scapula with intact skin. It is associated with upper
extremity fractures such as fractures of the scapula, clavicle, and humerus.
Most often, there are varying degrees of injury to the brachial plexus and the
subclavian artery, resulting in a flail and pulseless upper extremity. An arteriogram
should be performed to diagnose a vascular injury. A chest x-ray shows
significant lateral displacement of the scapula; however, the injury can be
missed!
First method of treatment consists of advanced trauma life
support (airway breathing, circulation), followed by an arteriogram for
evaluation of the vascular injury and repair of the arterial injury, if possible.
Fat Embolism
Fat embolism syndrome is a clinical diagnosis with
non-specific or insensitive diagnostic tests. This occurs in trauma patients
with multiple long bone fractures or pelvic fractures. Suspect fat embolism
syndrome with the appropriate signs and underlying risk factors. The clinical
signs usually develop within 24-72 hours of the injury. A fat embolism will
develop earlier than a pulmonary embolism. Early stabilization of the fractures
decreases the rate of incidence of this complication.
Major signs of a fat embolism include: confusion, agitation,
petechial rash—axillae, conjunctivae, palate, and shortness of breath. Minor
signs are listed as: tachycardia, fever, anemia, thrombocytopenia, and fat in
the urine. For a diagnosis of a fat embolism, there must be one major sign and
four minor signs, as mentioned above. Treatment of the fat embolism consists of
diagnostic tests—however these are non-specific and insensitive, supportive
treatment—such as intubation and oxygenation, and prevention (stabilization of
long bone fractures).
Femoral Fracture in the Multiply Injured Patient
In a multiply injured patient, early skeletal stabilization
of a femoral fracture within 24 hours results in decreased incidence of
pulmonary complications and fat embolisms. The effect of reamed intramedullary
nailing for femoral fractures on the incidence of pulmonary complications in a
multiply injured patient or patients with concomitant chest injury is
controversial. Multiple studies have shown that reamed intramedullary nailing
for the acute stabilization of femoral fractures in the multiply injured
patient with a thoracic injury did not increase the occurrence of pulmonary
complications. External fixation is indicated for early stabilization of femoral
fractures in severely injured patients as a form of damage control in
orthopedics and as a temporary bridge to femoral nailing. External fixation is
also indicated in the presence of an associated vascular injury requiring
stabilization before repair and in the presence of severe soft tissue injuries
with extensive contamination.
Hip fractures in an elderly patient
Nonoperative treatment in elderly patients with hip
fractures results a high complication rate including pneumonia,
thromboembolism, urinary tract infection, and decubitus ulcers, resulting in a
high mortality rate.
The mortality rate is 25% in the first year following the
fracture. Early surgery within 48 hours of an injury has been shown to be
associated with a decreased one-year mortality rate.
Dislocations occur more in total hip arthroplasty than in
hemiarthroplasty. Too much retroversion causes posterior dislocation. Total hip
arthroplasty is done is physiologically active elderly patients with a displaced
femoral neck fracture. Although it may increase the risk of dislocation, there
is a lower revision rate and a superior long term future outcome.
Failure of fixation
Quality and maintenance of reduction of the fracture is
important. Closed reduction can be attempted, however the reduction must be
anatomic. If it is not anatomic reduction, then open reduction should be done. Open
reduction can be done through an anterior approach or a Watson-Jones approach. When
the fixation fails, you can attempt to repeat ORIF or you may do prosthetic
replacement. It is important to note that in elderly patients, treatment of
displaced femoral neck fractures with screws may have failures and revision
rates of up to 40%.
Fracture Distal to the Fixation
This is probably due to screw placement at or below the
lesser trochanter and poor bone quality, especially if you start anteriorly and
not laterally. It is also possible that this may be due to the poor angle of
the screw fixation and multiple attempts at drilling or guide pins. Treatment
typically consists of a refixation of the femoral neck and the subtrochanteric
fracture.
Nonunion of the fracture
Femoral neck fractures are considered to be intracapsular
fractures which are at a high risk of developing a nonunion. The femoral neck
fracture is surrounded by synovial fluid and there is no extraosseous blood
supply, no periosteum, or callus formation. The fracture healing occurs by
intraosseous bone healing alone. It can present itself as groin or buttock
pain, pain with hip extension, or with weight bearing. It can occur in about 5%
of nondisplaced fractures and about 25% of displaced fractures. If it occurs in
an elderly patient, an arthroplasty must be done. If it occurs in a young
patient, a valgus intertrochanteric osteotomy. A vascularized fibular graft may
benefit the patient as well. Nonunion fractures occur more in the vertically
oriented fracture pattern with loss of reduction and varus collapse. In younger
patients, we may possibly reorient the fracture line to be more horizontal by
doing the osteotomy. Usually, the nonunion is apparent by about twelve month;
however, there may be trouble in seeing the nonunion due to the fact that there
is no periosteum and no callus in the femoral neck.
Medical Complications
There is an increased risk of DVT of up to 80%. Some form of
prophylaxis is indicated, both mechanical and pharmacological for the patient.
It is imperative to consult the medical team for co-management. The aim of
treatment is early immobilization of the patient with pulmonary toilet. There
is a high mortality rate in the elderly—approximately 30% in one year. A surgical
delay of more than 72 hours will increase the risk of one year mortality. After
completion of the treatment, treating the osteoporosis is needed to decrease
the incidence of other fragile fractures.
Osteonecrosis (AVN)
The patient will have groin, buttock, or proximal thigh
pain. It occurs in 10% of nondisplaced fractures and in 30% of displaced
fractures. AVN could occur due to interruption of terminal branch of the medial
femoral circumflex artery by the fracture. The medial femoral circumflex artery
is the predominant blood supply to the femoral head. Usually, AVN is diagnosed
by an MRI or it can be obviously on the x-ray. Not all cases of AVN develop
evidence of radiographic collapse. AVN can be clinically significant when it is
followed by late segmental collapse.
Late segmental collapse can be seen as early as 6-9 months
following the fracture, but it is usually recognized by the second year.
Segmental collapse can be excluded if it does not occur by the third year. AVN
may occur due to an increase in the initial displacement, increase in the time
to reduction, or nonanatomic reduction. Treatment for AVN in younger patients
with less than 50% femoral head involvement may qualify for a valgus
intertrochanteric osteotomy. A free vascularized fibular graft or a total hip
replacement may be considered if the involvement of the femoral head is more
than 50%. In an elderly patient, a total hip arthroplasty will probably be
necessary.
Penetration of the screws into the hip joint.
Another possible complication is the penetration of the
screws into the hip joint. The screws should be placed within 5mm of the
articular cartilage. You can use multiple fluoroscopy images to confirm that
there is no penetration. The screws must be parallel so that it can allow the
fracture to be compressed. Make sure the threads of the screws cross the
fracture site, otherwise the threads will distract the fracture. You may use
long threads or short threads based on the situation.
Shortening
Femoral neck shortening after fracture fixation with
multiple cancellous screws can be a problem. The healed femoral neck fracture
with shortening is usually associated with a poor functional outcome.
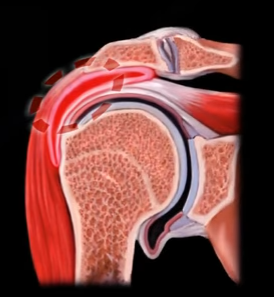
The acronym “PASTA”, stands for: Partial- The tear has not gone all the way through the tendon; Articular surface- the inner-side of
the tendon (not the bursal side); Supraspinatus
Tendon- tear on the underside of the
rotator cuff tendon; Avulsion- usually a traumatic injury which is caused by a pulling force.
PASTA lesions are difficult to diagnose but, an arthrogram
may help in the diagnosis. The tear can be seen on an ultrasound or an MRI. The
MRI arthrogram is done in the ABER position (abduction/external rotation) and
is more accurate in showing this lesion; the arm will be above the head in the
scanner.
A normal rotator cuff is about 10-12 mm in thickness. If
exposed bone between the rotator cuff and the articular margin is more than
7mm, then there is an at least 50% thickness tear—this is a classic indication
for surgery. When the lesion is less than 50% and painful, you can debride it.
If the lesion is more than 50% and painful, you can repair it. A physician may
complete a tear to become a full thickness tear, in order to repair it.
Rotator tears can be full thickness or partial thickness
tears. The partial can be a partial articular-sided supraspinatus tendon avulsion
(PASTA) which is an articular tear—the most common type. Another type of PASTA
tear—the Bursal Tear—also referred to as a reverse pasta lesion or, it could be
a Concealed Interstitial Delamination (CID) or an inter substance tear.
PASTA tears may be associated with internal impingement,
which is different than external impingement. In the external impingement there
is a subacromial impingement (bursal pathology). In internal impingement, the
pathology is on the under surface of the cuff, so PASTA tears may be associated
with the internal impingement.